The Joint Commission s Continuous Quality Improvement for Obesity
Release Notes:
Measure Information Form
Version 2022A
Measure Information Form
Measure Set: Health Care Staffing Services (HCSS)
Set Measure ID: HCSS-4
Performance Measure Name: Do Not Return - Per Diem
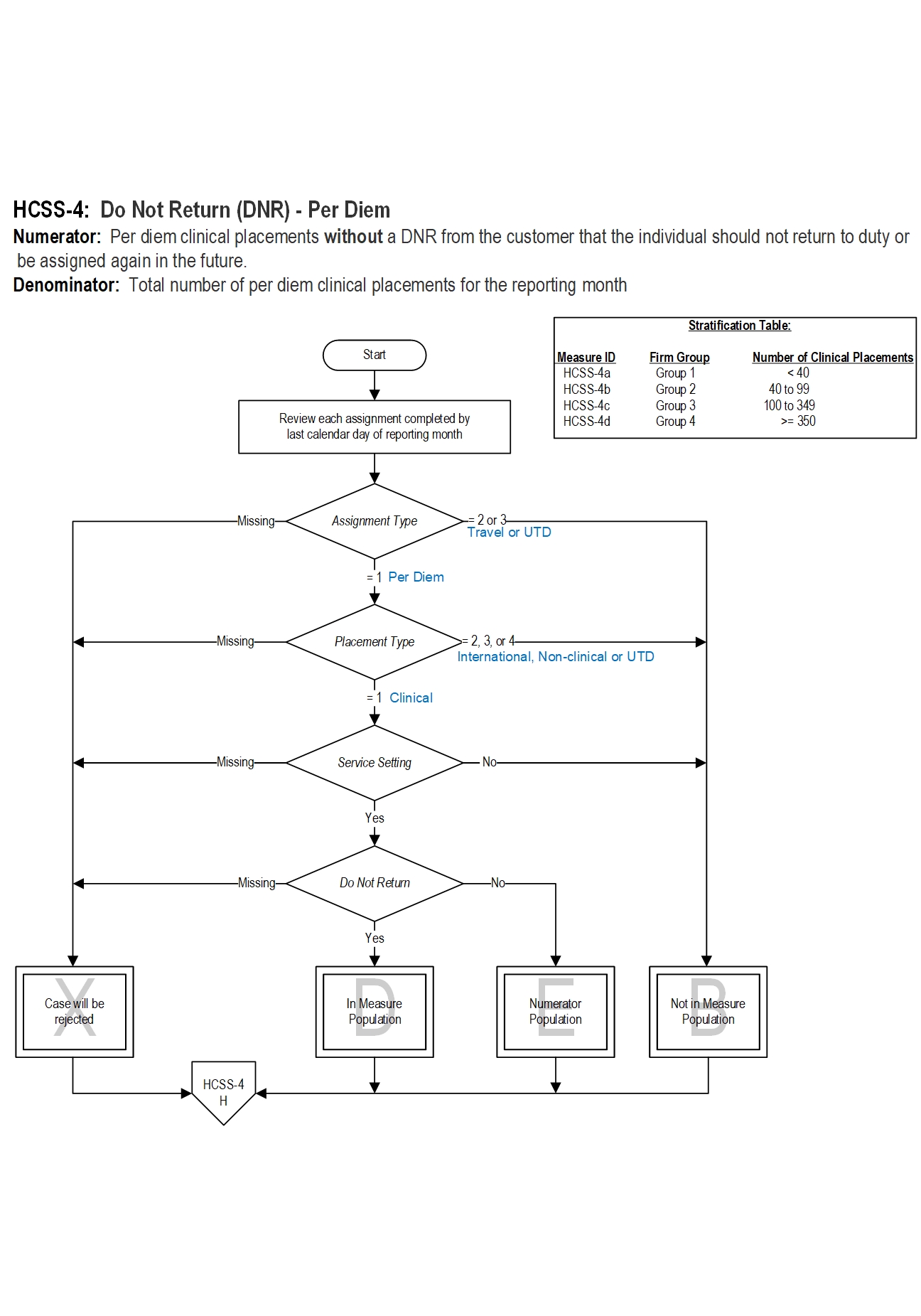
Description: This measure captures the proportion of per diem clinical placements that are not linked with a Do Not Return (DNR) from a customer. A DNR is defined as any customer request for an individual not to come back to complete the current assignment or be assigned in the future to a specific unit/ward of the facility, any unit/ward of the facility, or the entire health system.
The HCSS-4 measure is reported as a percentage which includes per diem clinical placements only. Firms may provide per diem staffing assignments only, travel staffing assignments only, or both per diem and travel staffing assignments. Data are reported monthly. NOTE: This measure is NOT reported by healthcare staffing firms with no per diem clinical staff.
Data are reported based on the size of the firm as determined by the total number of clinical placements identified for each site requesting certification in the certification application. The size of the firm is defined as the total number of clinical placements (i.e., employees) placed in a 12 month period by each site listed in the application, including allied health professionals, nursing professionals, and licensed independent practitioners (LIPs); excludes independent contractors, if the firm requested in its application that these individuals should not be included in the scope of the certification review.
The Joint Commission Connect® e-app should be used as a reference to select the appropriate size category for reporting. Only one category may be selected for each review cycle.
GROUP 1 < 40 clinical placements
GROUP 2 40 to 99 clinical placements
GROUP 3 100 to 349 clinical placements
GROUP 4 >= 350 clinical placements
Rationale: Health care staffing services (HCSS) are contracted to fill vacancies that health care organizations are unable to fill with currently employed staff. Client needs may be temporary due to staff turnover or retirement, backfill for sick days or vacation, seasonal or routine. According to a 2017 report from the Kaiser Family Foundation, 10% of the more than 3.3 million professionally active registered nurses in the United States are travelers (Kaiser, 2017). A 2017 Survey of Temporary Physician Staffing Trends revealed that 94% of healthcare managers had used a locum tenens physician during the last 12 months and 26% had used a nurse practitioner (NP) or physician assistant (PA), compared to 80% and 12.4% respectively in 2011-2012 (Staff Care, Inc., 2017). The demand for healthcare staffing services is expected to increase an average 7% per annum, including allied health professionals, per diem nursing, traveler nursing, and locum tenens (Harris Williams, Co., 2015). Temporary help employment growth averaged 3.9% over the first five months of 2017, with the highest level recorded for May at 4.9% (Thiyagarajan, 2017). Healthcare staffing services demand continues to grow as a result of an aging Baby Boomer population, an increased number of insured under the Affordable Care Act, healthcare professional shortages, and a push for lower nurse-to-patient ratios.
The use of temporary registered nurses and other temporary clinical staff is a common practice among U.S. hospitals and other healthcare facilities. Findings from several studies have found no evidence linking the use of temporary staff with positive or adverse patient outcomes, such as, in-hospital mortality, medication errors, falls, or patient satisfaction (Xue, et al., 2012; Aiken, et al., 2007). Qualitative studies of a mixed work environment comprised of permanent and temporary staff have described differences in perceptions, attitudes and behaviors between the two groups. For example, temporary staff may feel that they have fewer opportunities for continuing education and professional development while permanent staff may perceive heavier workloads related to administrative tasks (e.g., staff supervision, scheduling, developing policies and procedures, equipment maintenance, and planning activities with medical staff). Permanent staff may also see their compensation as less than the value they bring to the organization (Jansson and Engström, 2017). Furthermore, permanent staff may perceive temporary staff as a threat to their organizational status and self-esteem (Lapalme and Guerrero, 2019). Fair and equal management procedures and practices for both staffing groups (e.g., similar evaluation processes), may help promote team-work and limit counter-productive behaviors.
Joint Commission certified health care staffing firms should send quality temporary staff who are skilled and reliable to healthcare facilities; however, sometimes temporary staff performance may be less than satisfactory or does not meet customer expectations. When such instances occur, the customer may request that the individual not return for future assignments, e.g., "Do Not Return" (DNR). Reasons for DNR vary and may be due to clinical skills and competence, unprofessional behaviors, or perceptions that may be subjective, biased, or unjustified. Regardless of the reason underlying the request, DNR requests may negatively impact the business relationships and reputation of the firm. Firms should develop processes to prevent and manage DNR occurrences.
Ade-Oshifougun and Dufelmeier (2012) used Rampersad's six-step continuous quality improvement process to identify recurring problems and causes of DNR incidents. The team identified two objective reasons for DNR: poor quality of care; and, lack of orientation to and knowledge of specialty units. In addition, they developed educational tools that firms can use to proactively manage and prevent or decrease the number of DNR notices. "Prevention is key to reducing DNRs…and should be started before the hiring process and continued throughout".
Type Of Measure: Outcome
Improvement Noted As: Increase in the rate
Numerator Statement: HCSS-4: Per diem clinical placements without a DNR from the customer that the individual should not return to duty or be assigned again in the future.
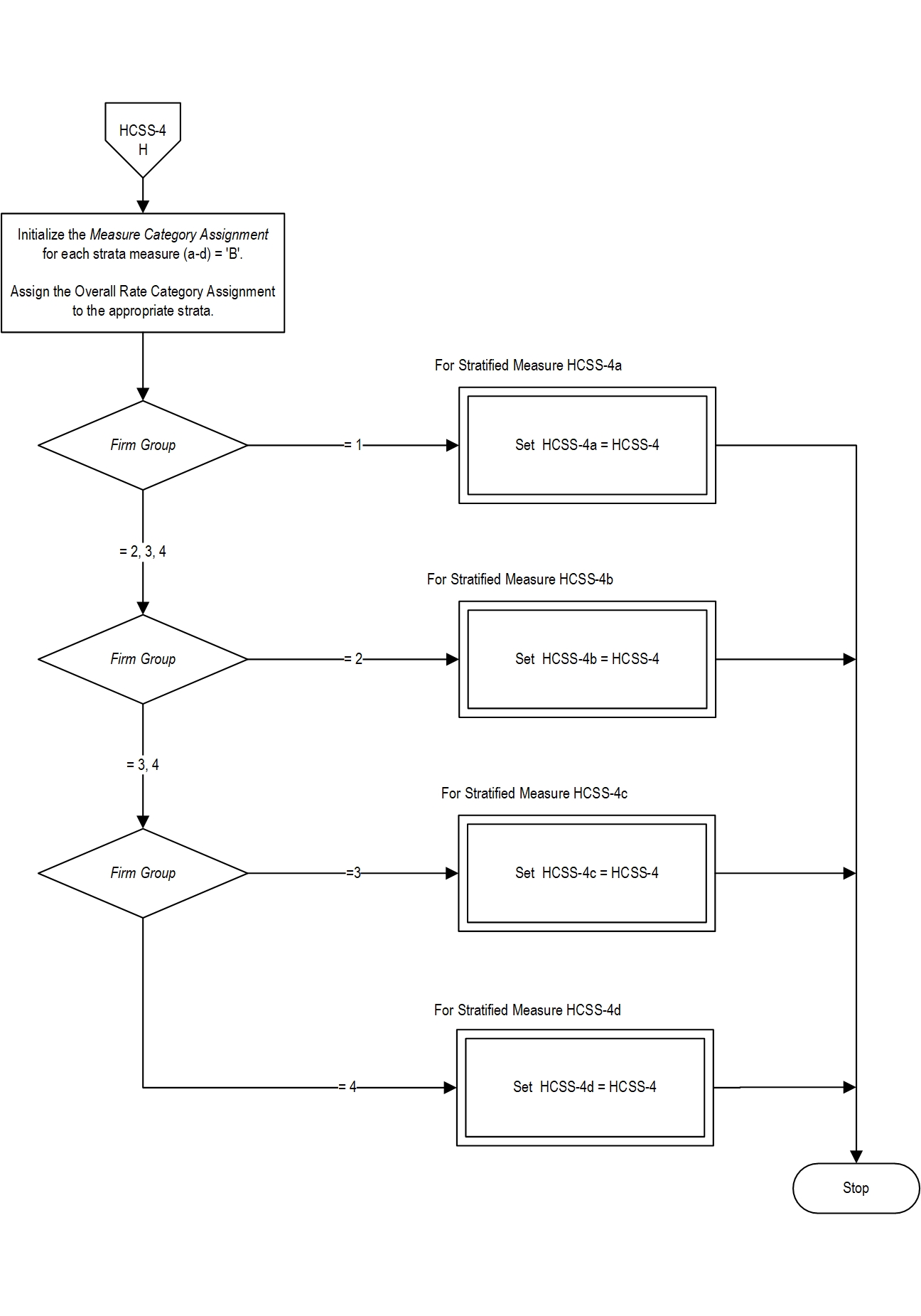
HCSS-4a Firms in Group 1: Per diem clinical placements without a DNR.
HCSS-4b Firms in Group 2: Per diem clinical placements without a DNR.
HCSS-4c Firms in Group 3: Per diem clinical placements without a DNR.
HCSS-4d Firms in Group 4: Per diem clinical placements without a DNR.
Included Populations: Not applicable Excluded Populations:Data Elements:
- Clinical employees who are ineligible for hire, rehire, or placement of any kind, e.g., Do Not Use (DNU)
- Cancellations due to customer need for temporary staff
- Do Not Return
Denominator Statement: Total number of per diem clinical placements for the reporting month.
Included Populations: NoneExcluded Populations: None
- Per Diem assignments, AND
- Clinical placements, AND
- Placements in a Service Setting
Data Elements:
- International placements
- Non-clinical placements
- Travel staff assignments
- Assignment Type
- Firm Group
- Placement Type
- Service Setting
Risk Adjustment: N/A.
Data Collection Approach: Retrospective data sources for required data elements include administrative data and, if applicable, medical record documents. Concurrent and retrospective data sources for required data elements include administrative (electronic) databases or hard copy (paper) records and files.
Data Accuracy: Variation may exist in electronic software tools used by healthcare staffing firms; therefore, specific data fields used to abstract DNR alerts may require evaluation to ensure consistency.
Measure Analysis Suggestions: Data should be used to evaluate reasons for DNR and develop a plan to improve employee performance.
Sampling: No.
Data Reported As: Aggregate rate generated from count data reported as a proportion.
Setting: Health Care Staffing Services
Report Period: Quarterly with monthly data points
Selected References:
- Ade-Oshifogun JB, Dufelmeier T. Prevention and Management of "Do Not Return" Notices: A Quality Improvement Process for Supplemental Staffing Nursing Agencies. Nursing Forum. 2012 April-June;47(2): 106-112.
- Aiken LH, Xue Y, Clarke SP, et al. Supplemental Nurse Staffing in Hospitals and Quality of Care. J Nurs Adm. 2007;37(7-8): 335-342.
- Harris Williams & Co. Healthcare Staffing Market Overview, November 2015.
- Jansson AB, Engström A. Working Together: Critical Care Nurses Experiences of Temporary Staffing Within Swedish Health Care: A Qualitative Study. Intensive and Critical Care Nursing. 2017;41: 3-10.
- Kaiser Family Foundation, April 2017.
- Lapalme ME, Doucet O. The Social Integration of Healthcare Agency Workers in Long-Term Care Facilities: A Cross-Sectional Study. International Journal of Nursing Studies. 2018;82: 106-112.
- Lapalme ME, Guerro S. How Do I Stand Compared to Agency Workers? Justice Perceptions and Employees' Counterproductive Work Behaviours. J Nurs Manag. 2019;27: 1471-1478.
- Staff Care, Inc. 2017 Survey of Temporary Physician Staffing Trends.
- Thiyagarajan S. Uptick in 2017. Staffing Industry Review. 2017 July/August;22(5): 12-13.
- Xue Y, Aiken LH, Freund DA, Noyes K. Quality Outcomes of Hospital Supplemental Nurse Staffing. J Nurs Adm. 2012 December;42(12): 580–585.
Measure Algorithm:
Source: https://manual.jointcommission.org/releases/HCSS2022A/MIF0123.html
0 Response to "The Joint Commission s Continuous Quality Improvement for Obesity"
Post a Comment